Brain. 2017 Mar 1;140(3):617-627. doi: 10.1093/brain/aww350.
Distinct brain imaging characteristics of autoantibody-mediated CNS conditions and multiple sclerosis.
Jurynczyk M, Geraldes R, Probert F, Woodhall MR, Waters P, Tackley G, DeLuca G, Chandratre S, Leite MI, Vincent A, Palace J.
Abstract
Brain imaging characteristics of MOG antibody disease are largely unknown and it is unclear whether they differ from those of multiple sclerosis and AQP4 antibody disease. The aim of this study was to identify brain imaging discriminators between those three inflammatory central nervous system diseases in adults and children to support diagnostic decisions, drive antibody testing and generate disease mechanism hypotheses. Clinical brain scans of 83 patients with brain lesions (67 in the training and 16 in the validation cohort, 65 adults and 18 children) with MOG antibody (n = 26), AQP4 antibody disease (n = 26) and multiple sclerosis (n = 31) recruited from Oxford neuromyelitis optica and multiple sclerosis clinical services were retrospectively and anonymously scored on a set of 29 predefined magnetic resonance imaging features by two independent raters. Principal component analysis was used to perform an overview of patients without a priori knowledge of the diagnosis. Orthogonal partial least squares discriminant analysis was used to build models separating diagnostic groups and identify best classifiers, which were then tested on an independent cohort set. Adults and children with MOG antibody disease frequently had fluffy brainstem lesions, often located in pons and/or adjacent to fourth ventricle. Children across all conditions showed more frequent bilateral, large, brainstem and deep grey matter lesions. MOG antibody disease spontaneously separated from multiple sclerosis but overlapped with AQP4 antibody disease. Multiple sclerosis was discriminated from MOG antibody disease and from AQP4 antibody disease with high predictive values, while MOG antibody disease could not be accurately discriminated from AQP4 antibody disease. Best classifiers between MOG antibody disease and multiple sclerosis were similar in adults and children, and included ovoid lesions adjacent to the body of lateral ventricles, Dawson's fingers, T1 hypointense lesions (multiple sclerosis), fluffy lesions and three lesions or less (MOG antibody). In the validation cohort patients with antibody-mediated conditions were differentiated from multiple sclerosis with high accuracy. Both antibody-mediated conditions can be clearly separated from multiple sclerosis on conventional brain imaging, both in adults and children. The overlap between MOG antibody oligodendrocytopathy and AQP4 antibody astrocytopathy suggests that the primary immune target is not the main substrate for brain lesion characteristics. This is also supported by the clear distinction between multiple sclerosis and MOG antibody disease both considered primary demyelinating conditions. We identify discriminatory features, which may be useful in classifying atypical multiple sclerosis, seronegative neuromyelitis optica spectrum disorders and relapsing acute disseminated encephalomyelitis, and characterizing cohorts for antibody discovery.
Figure 1: Principal component analysis (PCA; statistical modeling) looking at subjects involved without a priori knowledge of their diagnosis. The MS adults are on the right-hand side in a majority of cases vs antibody-mediated disorders.
I guess you can't teach an old dog new tricks, but, you can give an old dog new toys. This is what Jurynczyk et al. have done, pulling together their imaging and biological expertise, coming to the conclusion that based on MRI appearances alone that you can differentiate MS from other autoantibody-mediated disorders (see Figure 1 above). So, what are their findings?
1) MOG (Myelin Oligodendrocyte Glycoprotein) disease and AQP4 (Aquaporin 4) disease.
The former targets MOG located on the outer layer of myelin, whilst, the latter targets Aquaporin on astrocytes. Despite, the different targets you cannot distinguish between the two.
They found 'fluffy' brainstem (the area between the forebrain and spinal cord) lesions and three lesions or less in MOG antibody disease (see Figure 2), which has not been described before. Moreover, children with this disorder frequently displayed large, bilateral brainstem and deep grey matter lesions (basal ganglia) than adults. Before, we knew about MOG, I remember putting these cases into the ADEM (Acute Demyelinating EncephaloMyelitis) category (again ADEM is an MRI diagnosis). The authors propose that using this new description can be used to diagnose MOG disease in centers where the antibody test is not available. I personally think this would lead to over- or mis-diagnoses, and as we use more targeted treatments in inflammatory disorders this may prove dangerous.
Figure 2: MRI brain lesions in MOG antibody disease. Arrows point to lesions located in (A) the right middle cerebellar peduncle in a 50-year old male; (B) the right middle cerebellar peduncle in a 34-year-old male; (C) pons and medulla, adjacent to fourth ventricle, in a 30-year-old female; (D) middle cerebellar peduncles bilaterally in a 37-year-old female; (E)
midbrain, pons, cerebellar peduncles and cerebellum, adjacent to fourth
ventricle, bilateral, large and poorly demarcated, in a 37-year-old
female; (F) fluffy large and bilateral lesions in pons
and cerebellar peduncles, adjacent to fourth ventricle, and in thalamus
in a 3-year-old male; and (G) fluffy bilateral basal ganglia lesions in a 14-year-old female.
Interestingly, they also found in NMO subjects with brain lesions during an attack were more likely to experience simultaneous transverse myelitis - 75% (called as such when inflammation involves the spinal cord) than optic neuritis - 50% (when it involves the eyes), suggesting a mode of spread for these antibodies (maybe via the venous plexus or the lymphatic system).
2. Multiple Sclerosis
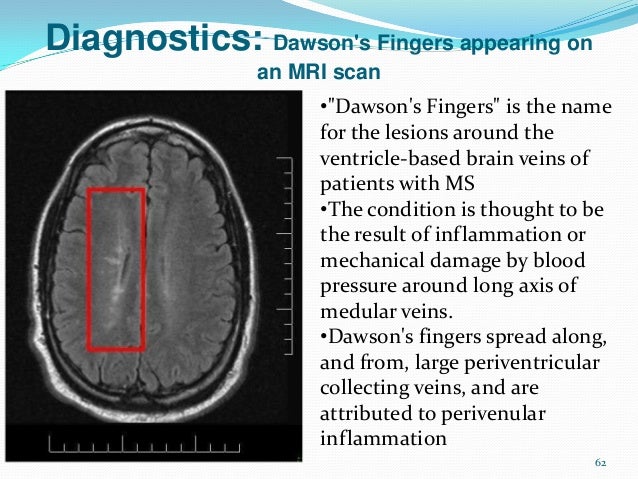
Features that differentiate MS from antibody mediated disorders include 'ovoid'/round lesions adjacent to the lateral ventricles and Dawson's fingers (see Figure 4). In children T1 black holes were also a helpful pointer towards MS (probably an indication of the regenerative capacity of the young brain from one-off antibody mediated attacks).
Figure 4: Dawson's fingers in MS
One of the failings of this paper is the lack of evaluation of the
'normal' MRI, as one of the biggest confounder's of white matter
lesions is the so-called small vessel ischaemic lesion (vascular strokes), which increases
with age. Equally, whether this guidance will prevent our neuroradiologists from
offering a differential of ADEM, MS, NMO and inflammation in general for the same case is a
debate for another day. Labels: MOG antibody disease, NMO and MS